
This article is Part 1 of the series ‘Addressing Maternal and Child Health Challenges’ I published with the Boston Congress of Public Health as a Thought Leadership Fellow
Salt, sugar and water. That’s all it could take to save a life. This combination, known as Oral Rehydration Solution (ORS)1, has been hailed by The Lancet as the most important medical advance of the 20th century. Between 1982 and 2007, it is estimated to have averted 50 million deaths due to diarrhea among children younger than five. While ORS does not cure or stop diarrhea, it replenishes lost fluids and salts, thereby preventing life-threatening dehydration.
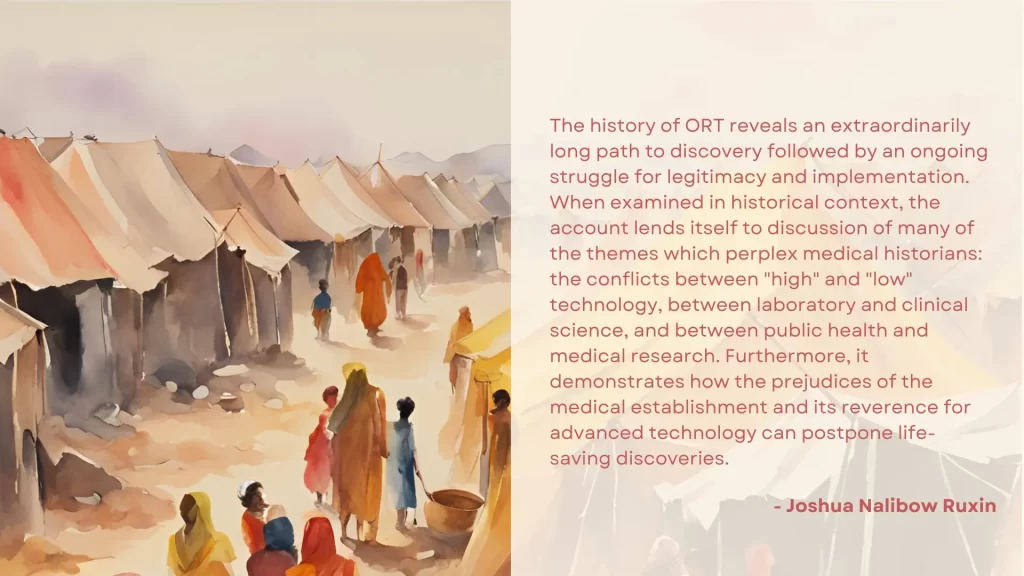
The treatment’s history is equally fascinating. While it had been used in clinical settings since the 1940s, Dr Dilip Mahalanabis was the first to deploy it at a large scale in field settings. During the Bangladesh war of 1971, 6,000 people were arriving in refugee camps in India every day, leading to overcrowding and cholera outbreaks.2 Without adequate intravenous saline solution or staff to administer it, Dr Mahalanabis and his team handed out ORS to the afflicted. The results were instantaneous and remarkable: mortality dropped from 30% to 1% in eight weeks.
Despite ORS being lauded as a ‘magic bullet‘, less than half of children with diarrhea received the treatment in 2022. By augmenting its use, we could potentially save an additional half a million lives a year.
Reasons for Low ORS Uptake
A systematic review of studies from 23 countries between 1981 and 2020 has analyzed the barriers and facilitators to ORS use. The review is fairly comprehensive, but given the long timespan and diverse locations it covers, not all the insights might be equally applicable to contemporary contexts or certain geographies. Availability, accessibility, and awareness have historically been major barriers, but over the years, many countries have made great strides in these respects. The study also points to the significance of design, adaptability, and cultural acceptability in interventions to promote ORS. Proper packaging and design can aid in the treatment’s correct use as well.
But even where ORS availability, access, awareness and demand are not challenges, ORS use can remain subpar.
A recent Science study in the Indian states of Bihar and Karnataka found that it remains underprescribed. The reason? Healthcare providers assume that people do not want ORS even though in household surveys, patients reported it as their most preferred treatment. Despite being aware of its life-saving potential, healthcare providers prescribed the treatment to only 55% of those who expressed a preference for ORS. Among those who did not state a preference, 28% received the treatment.
The study’s authors have identified reasons for the underprescription:
- Since the salts don’t cure diarrhea — they instead help avert dehydration — healthcare providers thought their patients wanted something more.
- Providers might think that patients would get ORS elsewhere (but they don’t).
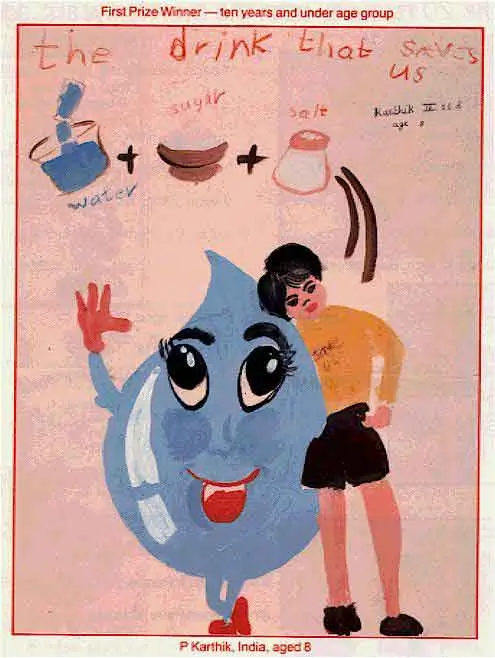
In this case, one could say that ORS is a victim of its simplicity. This has been true of the treatment since its inception (see image below), an aspect that is often overlooked in conversations around its use.
The Scourge of Simplicity
In this aspect, it reminds me of the public health intervention of washing hands before surgeries to prevent infections. In 1846, Hungarian doctor Ignaz Semmelweis found that doctors were transmitting infections to women in maternity wards by examining them after doing autopsies and that washing hands with chlorinated lime could prevent this. However, medical professionals derided him and his findings. While others echoed his claims, most notably Florence Nightingale, handwashing to prevent infections in medical settings became common only decades later.
In certain contexts, underwhelming perceptions of ORS have filtered down to patients, who might prefer other treatments over it. We can address these seemingly counterintuitive choices only if we understand the motivations behind them.
In her book Underbelly: Childhood Diarrhea and the Hidden Local Realities of Global Health, Rachel Hill-Clifford writes: ‘If families do pay and take the time to travel to a healthcare facility, they want to be compensated for their efforts with a treatment perceived as strong and effective. ORT is not perceived as such a treatment[…] What may be classified as unnecessary or “irrational”[…] in resource-constrained contexts such as Guatemala makes sense given limited accessibility of healthcare.’
With examples such as these, Hill-Clifford instantiates how larger equity and access issues can affect specific public health interventions, such as using ORS to treat diarrhea.
Strategies to Increase ORS Use
While ORS use is less than ideal at a global level and some countries have even seen a decline, others, such as Sierra Leone, Guyana, Malawi, and Bangladesh, have made remarkable strides in using it to cure diarrhea in children despite resource constraints. Both Guyana and Bangladesh achieved higher ORS coverage before their then wealthier neighbors, Trinidad & Tobago and India respectively.2
Some strategies that have been successful to increase
- Building demand among consumers and healthcare providers through the mass media, social marketing, one-on-one messaging, and other communication channels.
- Increasing the availability and access of ORS through both the public and private sectors.
- Free distribution of ORS by community health workers where price is a barrier.
Depending on the context, the solution could be deceptively simple. The Science study’s authors mention that since patients nudging doctors increased ORS prescriptions, just putting up a poster telling patients to ask for ORS rather than, say, antibiotics could be a way forward. Providers too thought it would give them more credibility when they prescribe ‘something as simple and basic as a pack of salts’.
However, there is no one-size-fits-all solution. What may have worked in one location might be unsuitable for another. When implementing strategies to increase ORS use — or for that matter, any public health intervention — it is important to understand the local context and social determinants of health so that we can accordingly fine-tune them.
Leave a Reply